Surgical paper I
Regular resection of left lateral lobe of liver for intrahepatic calculi
Introduction
Intrahepatic calculi, otherwise known as stones within the bile ducts situated above the left and right hepatic ducts, are an often underdiagnosed but significant clinical entity. Over the past five years, our hospital has recorded 368 cases of primary bile duct stones, which constitute 83.4% of the 441 cases of cholelithiasis surgeries performed during the same time frame. Of these, 112 cases were identified as intrahepatic stones, accounting for 30.4% of primary bile duct stone cases. These statistics align closely with domestic literature on the subject [4, 5]. However, it should be noted that the actual incidence is likely higher, given the limitations in diagnostic capabilities. The distribution of intrahepatic stones within the liver is further detailed in Table 1.
Table 1 Distribution of 112 Cases of Intrahepatic Stones
|
left + right hepatic ducts + biliary pore |
42 |
|
left + right hepatic ducts |
6 |
|
left hepatic duct + intracholedochus |
39 |
|
left hepatic ducts |
6 |
|
right hepatic ducts + biliary pore |
14 |
|
Other |
6 |
Intrahepatic calculi present a unique challenge in diagnosis and treatment, often leading to misdiagnosis and unsuccessful interventions. Until recently, the condition has been marked by a cycle of recurrent episodes, multiple surgeries, and repeated failures in treatment.
In a concerted effort to enhance the treatment outcomes for intrahepatic calculi, our hospital initiated a new surgical approach. Between 1975 and 1976, we performed resections of the left lateral lobe of the liver in five patients. Following a period of 3 to 4 years of postoperative surveillance, the long-term therapeutic outcomes have been promising. This innovative approach has not only yielded good long-term curative effects but also provided valuable insights that have significantly improved our treatment protocols for intrahepatic calculi.
Clinical Data
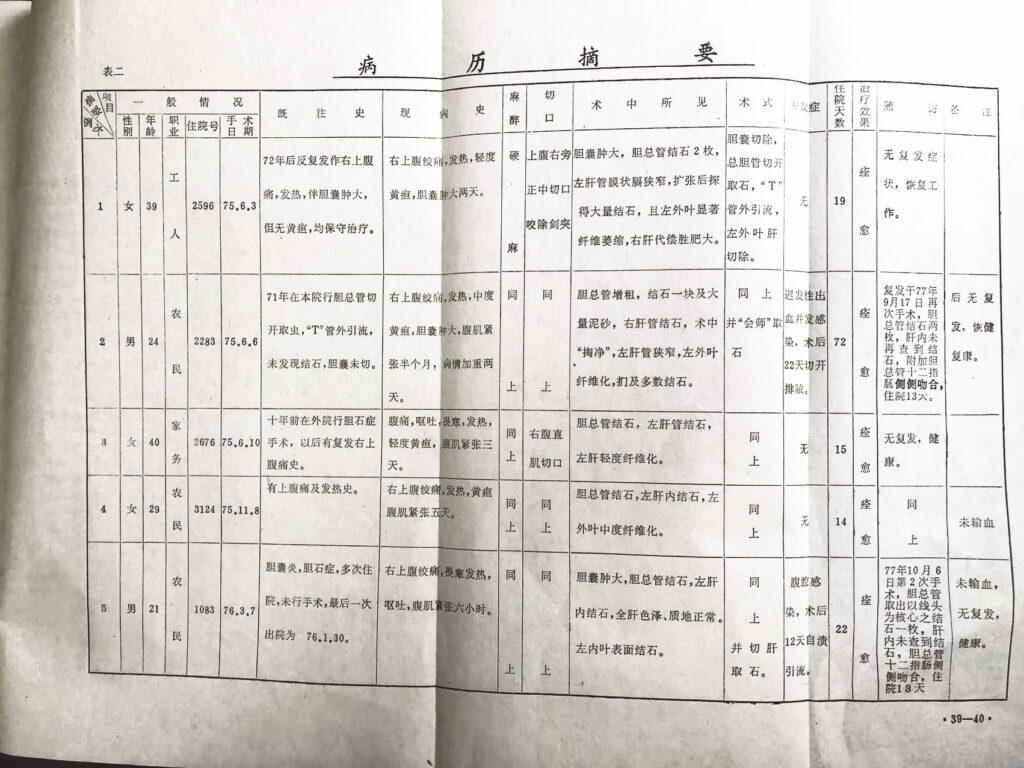
The study sample comprised a total of five patients: two males and three females, ranging in age from 21 to 40 years. Among them, two patients presented with residual stones. Intraoperatively, all cases were complicated by choledocholithiasis—stones in the common bile duct. The primary location for the intrahepatic calculi was identified as the left lateral lobe of the liver, where varying degrees of fibrous atrophy were also noted.
Surgical Procedure
All surgeries were performed under general anesthesia with abdominal incisions. Resection of the left lateral lobe was the principal surgical intervention. A "T"-shaped tube was employed for external drainage of the common bile duct, or additional intrahepatic calculi were extracted using a "joining forces" technique.
Postoperative Outcomes
Two cases experienced complications, specifically delayed hemorrhage and abdominal infection. The hospitalization duration for these patients varied between 14 and 72 days. However, all patients recovered fully and were discharged. Postoperative recurrence of choledocholithiasis was noted in two cases, necessitating further surgical intervention supplemented by a choledocho-duodenal lateral anastomosis. Subsequent examinations revealed no presence of intrahepatic bile duct stones.
Long-term Follow-up
All patients were followed for a period of 3 to 4 years postoperatively and showed no signs of recurrence. Overall health status was reported as good. (For a detailed summary of the original medical records, please refer to Table 2).
Diagnosis of Intrahepatic Calculi
The majority of surgeries for intrahepatic stones are performed to address biliary obstruction. Among the 112 cases in this group, 95 were complicated by common bile duct stones (84.9%). Previously, the removal of extrahepatic stones and restoration of biliary tract patency were considered sufficient for a "cure," supplemented by general treatment. However, this approach failed to account for potential adverse reactions arising from persistent intrahepatic infections. This oversight often resulted in repeated episodes and surgeries.
Diagnostic Methods
-
Intraoperative Indicators: If the common bile duct is expanded by pigment stones or filled with sediment and the gallbladder is clear of stones, this suggests hepatogenic stones, warranting further examination of intrahepatic lesions.
-
Visual and Tactile Examination: The liver's surface may exhibit localized hardness, paleness, and dome-shaped prominence, along with localized atrophy. In contrast, healthy liver tissue may show compensatory hypertrophy.
-
Liver Abscesses: Multiple bile duct-derived liver abscesses often indicate intrahepatic calculi.
-
Angiographic Evidence: "T" angiography may reveal negative shadows, such as a bean-and-pod pattern, suggesting intrahepatic stones.
-
Postoperative "T" Tube Drainage: The presence of sediment-like stone deposition in the drainage bottle indicates a reduction in postoperative intrahepatic stones.
The Role of Left Extrahepatic Lobectomy in Treatment
-
Minimal Surgical Trauma: This procedure inflicts moderate damage on liver function and minor disturbance on the body overall. When executed correctly, it solves most treatment challenges related to intrahepatic stones, ensuring short-term recovery and long-term satisfaction.
-
Complete Elimination: It eradicates lesions and prevents ongoing infections and stone reformation due to poor drainage and bile retention.
-
Alternate Exploration: The surgery allows for the exploration and removal of stones from other hepatic lobes, offering a different vantage point for tackling intrahepatic lesions.
-
Convenience: Compared to intrahepatic cholangiojejunostomy, left lateral lobe hepatectomy is technically easier to perform.
However, it's crucial to note that simpler surgical interventions are more suitable for patients with toxic shock, severe systemic infections, or extremely compromised liver function. Relief of obstruction is better achieved with "T" external drainage.
Surgical Indications
The following cases are considered appropriate candidates for the surgical resection of the left lateral lobe of the liver for treating intrahepatic calculi:
-
Multiple Intrahepatic Stones in the Left Lateral Lobe: Particularly when accompanied by fibrous atrophy, and when other hepatic lobes either have no stones or have stones that can be completely removed by other methods.
-
Calculus in the Outer Lobe with Poor Drainage: Cases where the outer lobe has calculus, along with bile duct stenosis and poor drainage, making it likely that stone regeneration will occur if only the liver parenchyma is cut open for stone removal.
-
Inaccessible Calculus at the Junction: Cases where there is calculus at the junction of the left inner lobe hepatic duct that cannot be removed through other means.
-
Left Lateral Lobe Calculus with Abscess: Cases where an abscess is present along with the calculus in the left lateral lobe.
-
Necessity for Roux-Y Longmire Surgery: Cases where the extrahepatic bile duct cannot be located due to inflammation or adhesion, or is too narrow to be shaped, thereby necessitating a Roux-Y Longmire procedure (anastomosis between the intrahepatic bile duct and jejunum) for drainage.
Implementation Technique of Regular Left Lateral Lobectomy
Preoperative Preparations
- Anesthesia: Continuous epidural anesthesia is recommended.
- Positioning: Patients should lie on their back with their right side elevated.
- Incision: A right rectus abdominis longitudinal incision is advised. The xiphoid process is sufficient, and if necessary, the seventh costal arch can also be cut off and exposed through extrapleural enlargement.
Hemostatic Techniques
- Local Blocking Method: After freeing the left lateral lobe, an assistant holds it or presses it against the costal arch, and the surgeon performs resection with minimal blood loss. This was the method used in all 5 cases.
- Hepatic Portal Block Method: The hepatoduodenal ligament is freed, and the hepatic artery and portal vein are blocked for 15 minutes, then relaxed for 5 minutes. This can be done safely and repeatedly.
- Other Techniques: Liver forceps, rubber bands, and the mattress suture method were not used.
Surgical Procedures
- Ligament Resection: Cut several ligaments like the ligamentum cirrhosae, falciform ligament, left triangular ligament, left coronary ligament, and hepatogastric ligament.
- Vein Ligation: Place a needle 1 cm to the left of the second hepatic portal and ligate the left hepatic vein. Be careful not to damage the middle hepatic vein.
- Liver Capsule and Parenchyma: Cut the liver capsule 1 cm along the left side of the suspensory ligament and sever the liver parenchyma with a knife handle. The cut should be flat, not in a "V" shape, to avoid damaging the left inner vein.
- Vessel Ligation: Each vessel should be ligated individually.
- Stone Removal: The hepatic duct and common bile duct are jointly opened to remove the stones, followed by internal and external suturing or drainage.
- Final Steps: The mattress suture is limited to not crossing the suspensory ligament. Turn over the suspensory ligament to cover the liver section and fix it. Use subhepatic siphon drainage or negative pressure drainage.
Discussion
Stone Distribution and Diagnosis
The distribution of intrahepatic stones is not random but follows patterns influenced by anatomical and dynamic factors, particularly favoring the left lobe. Direct imaging techniques are ideal but may not always be practical, making clinical judgment during surgery crucial.
Left Lobe Calculus
Calculus in the left lobe often undergoes significant fibrous atrophy, losing much of its function. However, the anatomical boundary of this lobe is well-defined, facilitating a safer and more convenient hepatectomy.
Treatment Efficacy
Left lateral hepatectomy is effective in treating most hepatolithiasis issues. Chinese reports show a success rate of around 90%. There were recurrence cases, but these were not related to the liver, suggesting that more comprehensive internal drainage strategies might prevent such outcomes.
Treatment Goals
The key to treating intrahepatic calculi is to remove the focus, ensure drainage, and prevent new stone formation. Surgery alone may not be sufficient, and a multi-pronged approach involving other treatments may be needed to prevent recurrence.
Infections
Hepatolithiasis often comes with serious infections, which can lead to abdominal infections. Aseptic techniques should be strengthened to mitigate this risk. The use of intraoperative bile duct irrigation should be carefully considered as it can spread infections.
Blood Transfusion
The necessity of blood transfusion is not emphasized; for generally healthy patients, it can often be avoided.
Etiology
The high frequency of intrahepatic stones, particularly bile pigment sediment-like stones, is not yet fully understood. However, it appears to be linked to biliary ascariasis and subsequent infections by Gram-negative bacteria. These factors contribute to the formation of stones with various cores, like parasite cadavers, making it an important subject for preventive medicine.
Summary
The paper summarizes the treatment and follow-up of 5 patients who underwent left lateral lobectomy to address intrahepatic stones. It delves into the surgical indications, the benefits of this particular surgical approach, the techniques employed, and the precautions that should be taken. One of the key takeaways is the recommendation to combine left lateral lobectomy with other methods like "reunion" for stone removal or incisions in the liver parenchyma. Coupled with the establishment of "valveless" internal drainage, this multifaceted approach aims to eliminate infection and prevent the recurrence of stones. The paper concludes that this strategy offers a viable treatment alternative for the complex issue of intrahepatic stones.
References
- Qian, Wenzhi. Preliminary experience in treating hepatolithiasis by intrahepatic cholangiojejunostomy. Chinese Journal of Surgery 18221- 1965
- Meng, Xianmin. Hepatectomy. Shanghai Science and Technology Press, Shanghai 1965
- Han, Yongjian. Liver Surgical Anatomy. Shanghai Science and Technology Press, Shanghai 1963
- Huang, Zhiqiang. Hepatolithiasis and its treatment. Chinese Journal of Surgery. 91716-1961
- Ran, Ruitu. Surgical treatment of intrahepatic bile duct stones. Chinese Journal of Surgery, 9:216-1961
- Zhou, Hongquan. Discussion on etiology and treatment of hepatolithiasis. Chinese Journal of Surgery 50(8):501-1964
Li Mingjie, Department of Surgery, Nanling County Hospital
This article was published in Journal of Wannan Medical College, Wannan Medicine, 1980, 13:51 and Domestic Medicine Surgery Volume (Part 1), 1981, 39
from 肝左外叶规则性切除治疗肝内结石