orthopedic paper III
Surgical analysis of surgical paraplegia
Report of 14 cases
Abstract: The article reviews the surgical treatments and long-term follow-ups of 14 patients who experienced paraplegia due to surgical causes over the last 13 years. The outcomes were 10 cases recovered, 3 cases improved, and 1 case deceased. The article details the causes, pathology, and surgical methods, followed by discussions.
Causes Classification:
- Spinal Fractures: 7 cases
- Spinal Tuberculosis: 5 cases
- Intradural Tumors: 2 cases
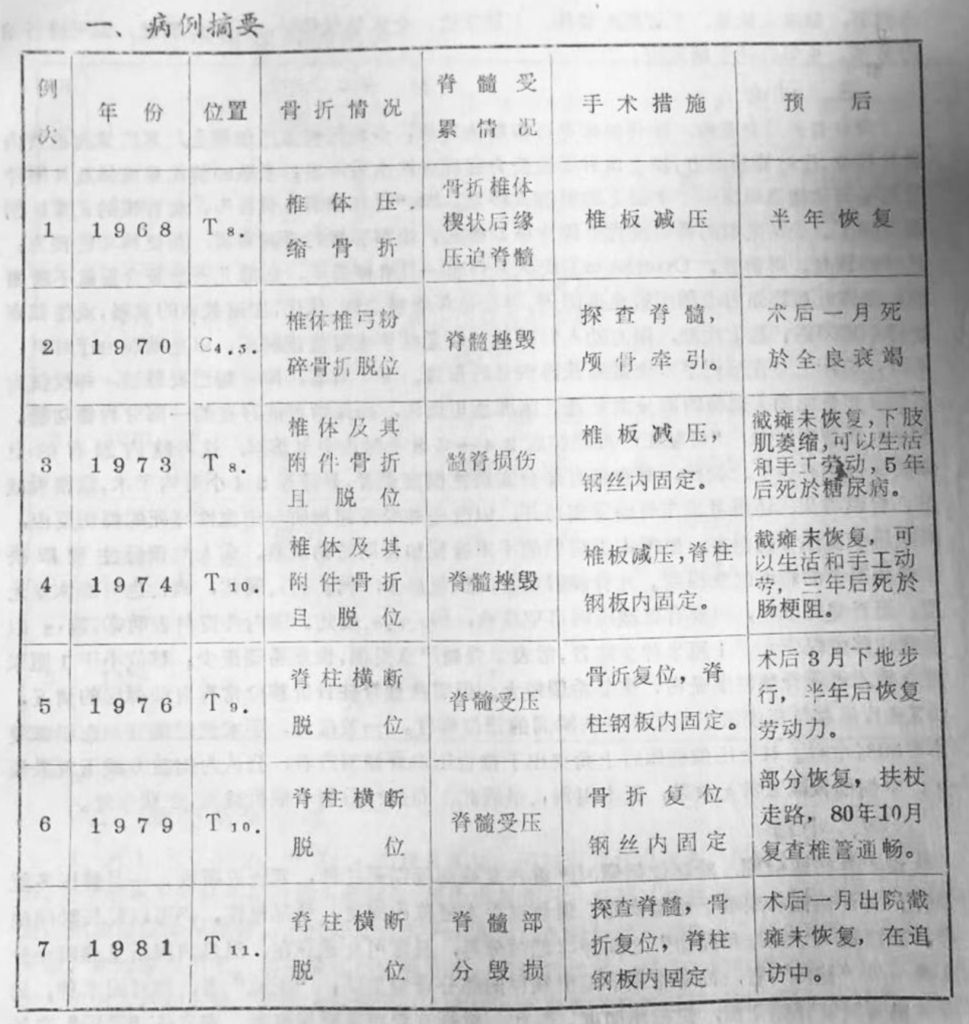
Spinal Fractures: Particularly in "complete transverse fractures" (refers to fractures affecting the vertebral body, arch, and intervertebral ligaments), dislocations are common. If it happens in the cervical-thoracic section, it often results in spinal cord contusions or compressions, causing paraplegia. Among them, 4 cases had spinal cord destruction observed during surgery, presenting as a mushy substance. No surgical methods could reverse the paraplegia. Apart from one case, which resulted in breathing difficulty and lung infection, leading to death one month post-injury, the rest could generally live for years with disabilities, even capable of manual labor.
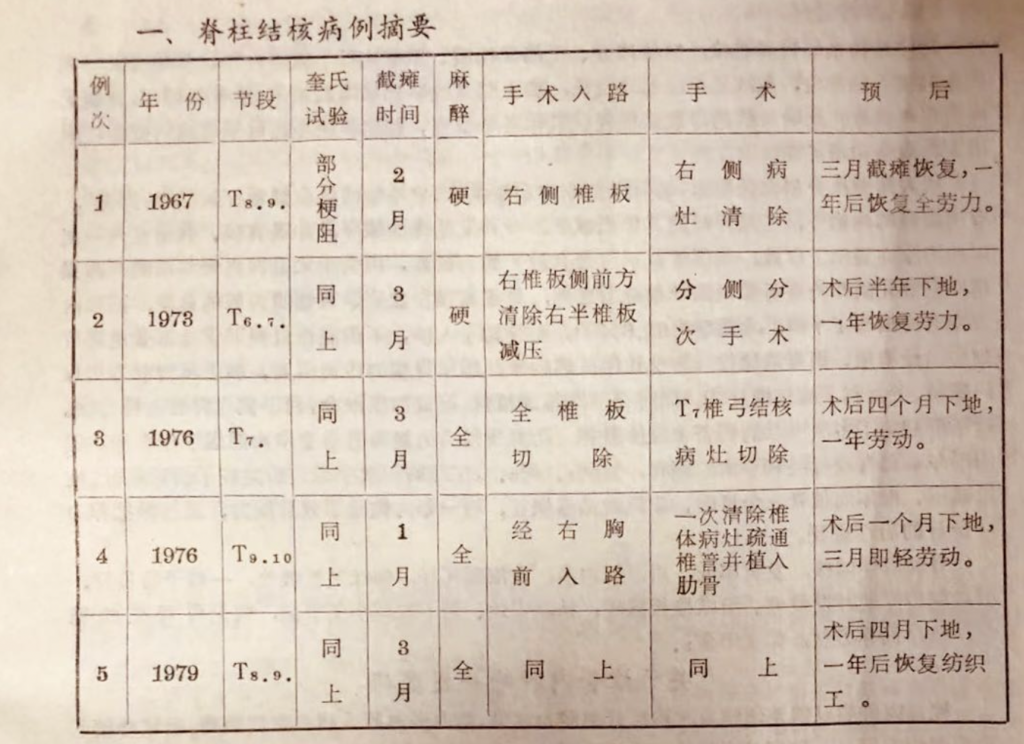
Spinal Tuberculosis: Especially in the thoracic section, due to the relatively narrow spinal canal and the inability for abscess to drain, it easily results in spinal cord compression and subsequent paraplegia. All 5 cases were in the lower thoracic section, 4 were vertebral tuberculosis, and 1 was arch tuberculosis. After surgical lesion removal, all recovered. The paper strongly recommends applying thoracic lesion removal and anterior intervertebral bone grafting in suitable cases, which not only increases the effectiveness but also significantly shortens the treatment period.
Intradural Tumors: Generally benign and located extramedullary. Surgery to remove or decompress shows good results. Both cases in this group were extramedullary benign tumors; one was completely removed, and one was mostly removed along with dural decompression, both achieving full recovery. However, surgery should be extremely cautious for malignant tumors to avoid accidental injuries and uncontrolled bleeding.
Overview
Spinal cord dysfunction due to injury or compression can result in varying degrees of paraplegia, which can have serious consequences for the patient. If managed appropriately, the majority of cases can be salvaged. Between 1968 and 1981, the author encountered 14 such cases, all of which underwent surgery, received a definitive diagnosis, and were given corresponding treatments. The outcomes were 10 cases fully recovered, 8 cases improved, and 1 case deceased. This paper introduces and analyzes the causes, pathology, surgical interventions, and prognoses of this patient group.
1. Classification of Causes
| Spinal Fractures | Spinal Tuberculosis | Intra-Spinal Canal Tumors |
| Spinal Cord Injury / Spinal Cord Compression | Vertebral Tuberculosis / Lamina Tuberculosis | Intradural Neurofibrom / Subdural Lipoma |
| 4 / 3 | 4 / 1 | 1 / 1 |
2. Degree of Paralysis
| Paralysis Index | 1 | 2 | 3 | 4 | 5 | 6 |
| Cases | 0 | 0 | 2 | 4 | 3 | 5 |
3. Choice of Anesthesia and Surgical Approach
Anesthesia |
Surgery |
||||
| Local Anesthesia | Epidural Anesthesia | General Anesthesia | Posterior Vertebral Approach | Anterolateral Approach | Anterior Trans-Thoracic Approach |
| 2 | 4 | 8 | 11 | 1 | 2 |
4. Surgical Methods
| Exploration + Traction | Exploration + Reduction + Fixation | Decompression + Reduction + Fixation | Lesion Removal + Decompression | Lesion Excision |
| 1 | 3 | 3 | 5 | 2 |
5. Pathological Changes and Prognosis
| Spinal Cord Injury (4 cases) | Spinal Cord Compression (10 Cases) | |
| No Change | died | Recovered |
| 3 | 1 | 10 |
Regarding Spinal Fractures Accompanied by Paralysis
Spinal fractures can appear at various segments of the spine due to different points of external force. However, because the spinal cord terminates at the lower edge of the first lumbar vertebra, below which is the cauda equina comprised of nerve fibers, its injuries are generally not complete. The spinal cord, on the other hand, is very delicate and easily damaged. As a result, the incidence of paralysis accompanying cervical and thoracic spinal fractures is high, and the prognosis is often poor.
The treatment objectives for these patients are:
- To explore the spinal cord, ascertain the pathological changes, and attempt to relieve compression or additionally take decompression measures, aiming to restore the vertebral canal's openness and make a prognosis.
- Under direct surgical view, to reset the fracture, take care to avoid repeated injuries, and apply strong internal fixation to restore the stability and supportive force of the spinal column.
For these purposes, although the work involves both orthopedics and neurosurgery, neither can be neglected. This is because the recovery of spinal cord function is a matter of life and death, while the recovery of spinal column stability is related to regaining labor capability. Both are often handled concurrently in clinical practice.
1. Case Presentation
2. Typical Case Introductions
Case 1: Male, 36 years old, had a complete transverse fracture and dislocation at the 9th thoracic vertebra. Palpation revealed spinal cord compression without destruction. Under direct vision, fracture reduction and decompression were performed, followed by internal fixation with spinal steel plates. Fourteen days post-surgery, the patient regained urinary function, lower limb muscle strength improved to Grade III, and sensation was restored. Discharged one month after surgery, the patient could walk with crutches in three months and gradually regained full mobility and working capacity. One year later, the steel plate was removed, and the patient was fully recovered.
Case 2: Cervical vertebrae 4 and 5 were shattered, and high-level paralysis was observed. Surgical exploration confirmed spinal cord destruction. Only cranial traction was applied. The patient died one month after surgery due to respiratory failure, lung infection, and bedsores leading to systemic collapse.
Case 3: Male, 42 years old, had a complete fracture at the 8th thoracic vertebra along with paralysis. During surgery, the spinal cord was found to have a mushy appearance. Spinal steel plates were used for internal fixation. Paralysis was not reversed; the muscles in the lower limbs atrophied, while the upper limbs developed. The patient relied entirely on crutches for mobility and had a reflexive bladder but could perform weaving work. He died five years later due to diabetes.
3. Discussion
Spinal fractures accompanied by paralysis pose significant risks. Aside from spinal shock that can recover over time, a few cases arise from vertebral compression causing the rear edge to move backward, compressing the anterior part of the spinal cord. This is often exacerbated by hematomas and reactive edema of the spinal cord. More commonly, the vertebral bodies and their attachments are injured or dislocated in a single plane, causing a "complete transverse fracture of the spine," which disrupts the normal anatomy of the spine. This leads to bone or bone fragments easily damaging and severing the delicate substance of the spinal cord, resulting in function loss that is difficult to recover.
Osterholm believes that once the spinal cord is mechanically compressed, local catecholamine levels increase, causing vascular constriction and blood supply obstruction in the affected area, thus accelerating the development of paralysis or making it irreversible. Based on this theory, it is strongly advised to undertake emergency surgical decompression to avoid missing the treatment window. However, there have been reports of paralysis recovery following delayed surgery. For cases where the spinal cord is already damaged, the goal is merely to explore and avoid further iatrogenic injuries while preserving any remaining spinal function. Allem points out that the spinal cord usually dissolves within 24 to 48 hours after severe injury, which is related to the intrinsic autolytic process within the spinal cord. Therefore, surgery is best performed within 24 hours for patients with partial spinal damage.
According to our long-term follow-up observations, the prognosis primarily depends on the degree of pathological changes in the spinal cord. Recovery is rare for patients with a destroyed spinal cord, as in cases 2, 3, 4, and possibly 7. On the other hand, for those with compressed spinal cords, effective decompression can often lead to full recovery, as in cases 1, 5, and 6.
Studies have shown that displacements greater than 1 cm in the thoracic vertebrae above T12 with complete paralysis often indicate severe spinal cord injury, with little hope for recovery. Displacements less than 1 cm usually indicate mild spinal cord injury with better chances of recovery. However, it should be noted that spinal fractures often have an automatic recoil effect, making the actual displacement greater than what X-rays may show. Overall, the surgical group has a 50% higher recovery rate than the conservative treatment group.
4. Conclusion
Traumatic paralysis can lead to different outcomes. Aside from cases of high-level paralysis which can result in short-term death due to severe complications, paralysis caused by compression can often be reversed through decompression. However, recovery from spinal contusions is less likely. Through surgical repositioning and internal fixation to stabilize the spine, patients can still survive for a prolonged period. It's important to note that there's no clear boundary between "compression" and "contusion," as both can coexist. Moreover, what is observed visually may not be entirely accurate. Those with contusions can still hope to maintain some residual spinal function, while those suffering from compression may also experience worsening paralysis due to edema or localized ischemia. Therefore, individuals suspected of having spinal cord damage should be treated as if they are "compressed" for maximum salvaging.
Regarding Spinal Tuberculosis Complicated by Paralysis
Spinal fractures can appear at various segments of the spine due to different points of external force. However, because the spinal cord terminates at the lower edge of the first lumbar vertebra, below which is the cauda equina comprised of nerve fibers, its injuries are generally not complete. The spinal cord, on the other hand, is very delicate and easily damaged. As a result, the incidence of paralysis accompanying cervical and thoracic spinal fractures is high, and the prognosis is often poor.
Spinal tuberculosis is usually found in the vertebral bodies, with the appendages rarely affected, accounting for about 1%. Obstruction caused by tubercular matter in the spinal canal can lead to paralysis, often in the thoracic region where the spinal canal is relatively narrow.
The likelihood of thoracic vertebrae tuberculosis leading to paralysis is high, and conservative treatment not only prolongs bed rest but also offers minimal chances of recovery. The complications of paralysis are pressing and demand urgent attention. Thus, early surgery, after appropriate preparation, has become the modern consensus. Under the protection of anti-tuberculosis treatment, complete lesion removal to clear the spinal canal, coupled with bone graft fusion to stabilize the diseased spinal area, can achieve good results and prevent recurrence. All five cases in this group were cured through surgery.
1. Case Presentation
2. Typical Case Studies
-
Case 1: Male, 35 years old, tuberculosis of the 8th and 9th thoracic vertebrae accompanied by paralysis. After three weeks of anti-tuberculosis preparation, a staged, lateralized surgical plan was carried out. Initially, the lesion on the right side was removed under spinal anesthesia, extracting a large amount of pus, necrotic bone, and tubercular granuloma. Post-surgery, the paralysis showed signs of recovery, but urinary catheterization could not be removed. One month later, a second surgery was planned to remove the lesion on the opposite side and perform spinal fusion. However, the patient experienced a high fever (41°C) and convulsions under general anesthesia, forcing the surgery to be halted. The patient then refused further surgeries and was discharged for home care. Twenty days after returning home, the urinary catheter fell out on its own, and the patient began to urinate independently. Three months later, he was able to walk with crutches and returned to light work after six months. A year after the surgery, the patient carried his ill mother for 40 miles to the hospital, astonishing the surgeons!
-
Case 3: Male, 36 years old, tuberculosis of the 7th thoracic vertebra arch, accompanied by paralysis. Four months after total laminectomy, he was able to walk, and a year later, he also returned to work. This case had a spinal angiogram showing pseudolocation due to arachnoid adhesions; the lesion was located during surgery and confirmed pathologically post-removal.
-
Case 5: Female, 29 years old, worker, tuberculosis of the 8th and 9th thoracic vertebrae. The vertebrae had collapsed, causing kyphosis, accompanied by proliferative pulmonary tuberculosis and a healed dislocation of the right hip due to tuberculosis. She was frail and weighed only 42 kilograms. During her pre-surgical hospital stay, her paralysis worsened, and she showed uncontrollable symptoms of sepsis. Surgery was performed under endotracheal ether anesthesia. The lesion was removed through the right thorax in one go, 2.5 diseased vertebrae were excised, and anterior decompression was performed. Tubercular material was scraped out from within a 10 cm section of the spinal canal, revealing a pulsating dura mater. Two rib sections were implanted between the vertebrae. The surgical field was flushed, and the thoracic cavity closed as per routine. The patient had no postoperative complications, the paralysis was quickly relieved, and the body also recovered smoothly. She was able to walk after four months in bed and returned to textile work after a year. X-ray follow-up showed successful bone graft fusion, disappearance of paravertebral abscess shadows, and slightly blunted costal angles.
3. Discussion
Spinal tuberculosis is a specific infection characterized by the presence of tubercular granuloma, caseous material, and pus both inside and outside the spinal canal, especially around the spinal cord. In the narrow thoracic spine, the pus doesn't easily drain, and along with necrotic bone or intervertebral disc tissue, this leads to spinal canal obstruction and consequent paralysis. Tuberculosis sepsis at this stage can affect multiple organs, making the situation far more complex and difficult to manage compared to paralysis caused solely by mechanical compression.
The posterior approach for staged, lateralized lesion removal has been a standard procedure to date. Not only does it eliminate the lesion and break the "tuberculosis barrier," aiding in lesion healing, but it also allows for spinal decompression. This is particularly effective for the recovery of concurrent paralysis, as demonstrated in Case 1. However, the method carries a certain degree of uncertainty. The surgery is performed deep within the body where visibility is limited, requiring reliance on experience to achieve "relative completeness." There's also the risk of accidentally damaging blood vessels, the spinal cord, or internal organs. According to domestic reports, the surgical success rate is 61.6%.
In contrast, the anterior thoracic approach allows for a thorough and effective lesion removal under direct vision. It also removes destructive tubercular material from the spinal canal and relieves spinal cord compression. Combined with reliable anterior decompression of the spinal canal, it significantly aids in the recovery from paralysis. Performing anterior intervertebral bone grafting also promotes compression fusion and helps restore spinal stability. This approach not only avoids the pain and economic burden of multiple surgeries but also significantly increases the cure rate and shortens the treatment duration, as seen in Cases 4 and 5.
In cases of spinal accessory tuberculosis, which has a lower incidence rate and generally better prognosis due to abundant peripheral muscles and good blood circulation, lesions are usually absorbed naturally. However, paralysis can still occur in the thoracic section. Laminectomy for spinal decompression and lesion removal is relatively convenient if it doesn't compromise the small facet joints, as in Case 3.
4. Summary
In cases of traumatic paralysis, except for high-level paralysis, which often leads to early death due to severe complications, paralysis caused by compression often shows a good recovery rate once decompressed. On the other hand, recovery is generally more difficult in spinal cord contusions. However, surgical repositioning and internal fixation to stabilize the spine can still lead to prolonged survival.
It’s important to note that the terms "compression" and "contusion" are not strictly separate and often coexist. What is observed with the naked eye isn't always entirely accurate. Therefore, in cases identified as "contusion," the hope lies in maintaining the remaining functional portions of the spinal cord. For those identified as "compression," secondary spinal cord degeneration can occur due to edema or local ischemia, making the paralysis worse.
Hence, for patients suspected of having substantial spinal cord damage, treatment should be approached as if the spinal cord is "compressed" in order to maximize the chances of recovery.
Regarding Spinal Tuberculosis and Resulting Paralysis
Spinal tuberculosis predominantly affects the vertebral bodies, while appendages of the spine are less commonly involved, accounting for about 1%. When tuberculous material fills the spinal canal and causes an obstruction, it can result in paralysis, most commonly in the thoracic region due to the relative narrowness of the spinal canal there.
The likelihood of paralysis is quite high in cases of thoracic spinal tuberculosis. Conservative treatment doesn't yield significant improvement; not only does it require prolonged bed rest, but the chance of complete recovery is also extremely low. Complications from the resulting paralysis can be aggressive and need immediate attention. Therefore, the modern consensus leans towards early surgical intervention after adequate preparation.
Under the cover of anti-tuberculosis treatment, thorough removal of the lesion to unblock the spinal canal is recommended. Additionally, bone graft fusion to stabilize the affected spinal area can achieve good results and prevent recurrence. All five cases in this group were completely cured after surgical intervention.
1. Case Presentation
2. Case Studies Summary
-
Case 1: Male, 35 years old, affected at T8-T9
- After three weeks of anti-tuberculosis treatment, he underwent staged, unilateral surgery to remove the lesion on the right side. Postoperative evaluation showed some recovery of paralysis, but a catheter for urination was still necessary.
- A second surgery for the opposite side was planned, but had to be stopped due to high fever and seizures under anesthesia. The patient opted out of additional surgeries and was discharged. After returning home, he started to urinate on his own within 20 days, and six months later, he was able to perform light work. Astonishingly, a year after the surgery, he even carried his sick mother 40 miles to the hospital.
-
Case 3: Male, 36 years old, affected at T7
- Four months after undergoing decompression of the entire vertebral arch, he could walk. A year later, he resumed work.
- Spinal angiography was performed, revealing false localization due to arachnoid adhesions. The lesion was identified and removed during the surgery and confirmed through pathology.
-
Case 5: Female, 29 years old, worker, affected at T8-T9
- Also suffering from proliferative pulmonary tuberculosis and a healed form of tuberculosis in the right hip, she weighed only 42 kg.
- During the preoperative preparation period, her paralysis worsened and septicemia symptoms could not be controlled. She underwent surgery, including removal of 2.5 affected vertebrae and spinal decompression.
- After the surgery, she experienced no complications, her paralysis was quickly resolved, and she returned to her textile work within a year. Radiography confirmed bone graft fusion and the disappearance of paravertebral abscesses.
Discussion Summary
-
Complex Nature of Spinal Tuberculosis
- The disease involves a unique type of infection where tuberculous granuloma, caseous material, and pus accumulate both inside and outside the spinal canal. This is more problematic in the thoracic spine, which is relatively narrow. Along with necrotic tissue and bone, this leads to spinal canal obstruction and paralysis. In addition, systemic symptoms due to tuberculosis further complicate the condition.
-
Surgical Approaches
- The standard surgical procedure involves staged, unilateral lesion removal via a posterior approach. This not only clears the lesion but also breaks the "tubercular barrier," aiding in healing. It's also effective in relieving paralysis, as in Case 1. However, the procedure is risky due to its "blind" nature.
- The anterior approach via the chest allows for a more effective and safer removal of the lesion under direct vision. It also offers the opportunity for reliable spinal decompression, aiding in the recovery of paralysis. Coupled with anterior interbody bone grafting, it enhances spinal stability.
-
Rate of Success and Adaptation
- Studies have shown a 61.6% success rate for the posterior approach. The anterior approach not only minimizes the pain and economic burden of multiple surgeries but also significantly improves the cure rate and shortens the treatment period. The authors are leaning towards adopting this approach, as in Case 4 and Case 5.
-
Attachments of the Spine
- Tuberculosis of the spinal attachments is rare and generally has a good prognosis due to good blood circulation and muscle mass around it. Even in the thoracic spine, where paralysis can occur, laminectomy and lesion removal without destroying the facet joints can achieve good results, as shown in Case 3.
Regarding Spinal Canal Tumors Complicated with Paralysis
-
Types of Tumors
- Most commonly found are meningiomas in the extradural intrathecal space.
- Gliomas and ependymomas are usually present within the spinal cord.
- Subarachnoid lipomas are relatively rare.
-
Mechanism of Paralysis
- The tumor creates a space-occupying lesion, putting pressure on the spinal cord.
- As the tumor grows, the paralysis progressively worsens.
- Non-surgical decompression or shunting is usually not effective in reversing this condition, highlighting the need for attention to these cases [7].
-
Differential Diagnosis
- It's crucial to distinguish these tumors from other conditions causing paralysis, such as transverse myelitis, and subarachnoid hemorrhage to avoid unnecessary surgery and complication.
1. Case Presentation
| Year | Spinal Segment | Queckenstedt's Test | Pathological Diagnosis | Surgical Findings | Surgical Method | Prognosis | |
|---|---|---|---|---|---|---|---|
| 1 | 1969 | T10 | Partial obstruction | Neurofibroma | T10 right paraspinal, extradural, intrathecal mass of 1.5×1.0x1.0 cm | Complete Tumor Excision | Recovered (2 months) |
| 2 | 1979 | C7 T1 | Complete obstruction | Subdural Lipoma | C7 T1 subdural lipoma compressing the spinal cord by 50%, length 3 cm | Partial Tumor Excision (~70%), Dural Decompression | Recovered (6 months) |
Case 1: A neurofibroma located at the T10 spinal segment was completely excised. The Queckenstedt's test showed partial obstruction. The patient recovered in 2 months. Straightforward and effective, like a clean piece of code.
Case 2: This one's a bit more complex. A subdural lipoma at C7 T1 caused complete obstruction. About 70% of the tumor was removed and the dura was decompressed. It took 6 months for the patient to recover, but hey, they did recover!
Discussion
Clinical Confirmation
Both cases were diagnosed through clinical neuro-localization, confirmed during surgery. It's like finding a bug in a specific part of the code—difficult but not impossible.
Pre-operative Uncertainty
It was hard to nail down the pathology before surgery, but both cases improved post-operation. The first case was easier to handle with complete tumor excision since the neurofibroma was outside the spinal cord. The second case required a more cautious approach: the benign lipoma was intimately adhered to the spinal cord, so only partial removal was attempted. They also decompressed the dura to relieve pressure.
The Root Cause
The root cause of spinal cord paralysis due to tumors is essentially mechanical compression within the spinal canal. Similar to an overloaded server, the only solution is to alleviate the congestion. Various diagnostic tests like cerebrospinal fluid dynamics and chemical examination can help confirm this.
Diagnostic Methods
Spinal angiography can theoretically localize the lesion, but like any sophisticated AI model, there can be false positives or negatives. Clinicians must consider errors, adhesions, vascular anomalies, and other factors.
Importance of Pre-op Assessment
Efforts must be made to understand whether the tumor is inside or outside the spinal cord, benign or malignant, as this influences both the surgical complexity and prognosis. It's like optimizing an algorithm—you need to know the variables affecting the output.
Urgent Action
If the diagnosis is unclear, it's better to operate sooner rather than later. First, most spinal tumors are benign and easier to treat. Second, even if it's malignant, at least you can relieve the pressure. But caution is crucial; surgeries aren't risk-free. Third, surgical and pathological examinations can confirm the diagnosis, allowing for appropriate management.
Summary
Long-Term Observations
The study recaps 14 cases of paralysis due to surgical causes over a 13-year span. It's like looking back at 13 years of software updates—some work wonders, some need patching. Various treatment methods were evaluated and outcomes of individual cases were discussed.
Outcomes
Of the 14 cases, there were no surgical mortalities. Ten fully recovered; one with a high cervical injury died shortly after surgery; one case is too recent for assessment; two more lived for 5 and 3 years post-operation but eventually died due to complications like diabetes and intestinal obstruction, making it unclear if their paralysis contributed to their deaths.
Tuberculosis and Benign Spinal Tumors
100% effective treatment was shown here. It's like finding that perfect algorithm you've been dreaming about. Treatment for thoracic spine tuberculosis-induced paralysis has significantly advanced, reducing treatment time and increasing the chances of successful outcomes. So, we're overcoming historical fears.
Key Takeaways
For traumatic spinal paralysis, the severity of the spinal injury is the key determinant for outcomes—just like how the root cause of a bug determines how messy the debugging is going to be.
References
- Guo Shi Fu et al.: "Preliminary Observations on Pathological Changes After Spinal Injury and Different Treatments (Animal Experiments)," Bone Supplement: 4:176, 1979
- Xu Shao Ting: "Early Treatment of Earthquake-Induced Spinal Fractures and Spinal Injuries," Orthopedics Supplement: 4:146, 1980
- Guo Ju Ling et al.: "Preliminary Summary of Treatment for Earthquake-Induced Paralysis," Orthopedics Supplement: 1:28, 1978
- Fang Xian Zhi et al.: "Lesion Removal Therapy for Tuberculosis of the Joints and Bones," P: 58 (People’s Health Publishing House) 1957
- Fan Bing Zhe: "Thoracic Lesion Removal Surgery for Thoracic Tuberculosis," Chinese Journal of Surgery: 7:20, 1959
- Wang Zhi Xian: "Thoracic Cavity Lesion Removal Surgery for Spinal Tuberculosis," Chinese Journal of Surgery: 7:271, 1959
- Zeng Guang Yi et al.: "Spinal Tumors," Chinese Journal of Surgery: 10:(6)374, 1962
- Wu Ying Kai et al. (Trans.): "Soviet War Medical Experience, Selected Translations in Surgery," Volume 11, People’s Health Publishing House: 1956
This article was originally originally published in the proceedings of the Second Orthopedic Academic Conference in Anhui Province; initial draft was written in January 1981 and later revised in September 1981 Nanling Hospital, Li Mingjie Note: This article has been reviewed by Dr. Yuan Sizhong from the Orthopedic Department of Wuhu District Hospital, to whom we extend our special thanks.
from 外科截瘫14例手术分析