Surgical paper VIII
Biliary enteric drainage
Literature Review and Clinical Analysis
Abstract
Between 1974 and 1980, a comprehensive review was conducted on 441 biliary duct surgical procedures, which included 81 instances (18%) of Internal Biliary-Intestinal Drainage (IDBI). This subset featured 61 cases of choledochoduodenostomy, 15 of Oddi's sphincterotomy, 2 hepatocholangiojejunostomies in the Roux-en-Y configuration, 2 Brown-type choledochojejunostomies, and one instance of U-type biliary-intestinal bridging.
The patients in this cohort generally experienced good health post-surgery, with no significant symptoms or signs of reflux. However, two exceptions were noted: one patient died due to an infection in the U-bridge, and another experienced recurrent cholelithiasis following a Finster's technique procedure, necessitating re-operation.
This paper places particular emphasis on the issue of postoperative reflux in the application of IDBI for treating biliary tract obstructions and cholelithiasis. Advances in diagnostic and therapeutic techniques, including ultrasound, CT scans, endoscopy, percutaneous transhepatic cholangiography (PTC), and endoscopic retrograde cholangiopancreatography (ERCP), have considerably evolved the landscape of biliary tract disorder management.
Keywords:
Internal Biliary-Intestinal Drainage, Sump Pool Syndrome, Cholelithiasis
Introduction
Over the past six decades, advancements in various diagnostic techniques—particularly in Bus, PTC, ERCP, and CT—alongside animal clinical trials and in-depth research into biliary pathophysiology, have led to a renewed understanding of Biliary Enteric Drainage (BID). While the topic remains a subject of ongoing debate, it is clear that the field is moving along a path of increasing maturity and depth.
The concept of duodenal papillotomy has evolved significantly since its initial proposal in 1884. Despite a century of continuous exploration and advancement, a standardized surgical procedure for Biliary Enteric Drainage (BID) has yet to be established. The selection of surgical indications and technical nuances often depends on a myriad of factors—ranging from the specific clinical condition and the surgeon's individual expertise to the available equipment.
For the purposes of this study, we have reviewed a sample set comprising 441 cases of biliary surgery conducted in the Nanling region between 1974 and 1980. This data has been analyzed in conjunction with existing literature to provide a comprehensive review of BID.
Applications of Biliary-Enteric Internal Drainage (BID)
1. Restoring Normal Bile Flow
In cases where the bile-intestinal pathway is interrupted or narrowed due to tumors or injuries, BID aims to restore normal bile flow. This involves creating an artificial channel as an alternative route for bile to pass through.
2. Post-Surgical Bile Flow Management
After surgical corrections for conditions such as intrahepatic and extrahepatic bile duct stones or bile duct stenosis, BID is employed as a preventive measure. The objective is to maintain smooth bile flow, thereby preventing complications like bile stasis, recurrent infections, and further formation of stones.
On "Reflux Infections" and "Blind Bag Syndrome"
Concerns About Reflux
All Biliary-Enteric Internal Drainage (BID) procedures inherently disrupt the physiological function of the sphincter of Oddi, effectively eliminating the natural "valve" mechanism between the biliary and intestinal tracts. While the general flow direction of bile into the intestine is facilitated by factors like gravity, pressure, and peristaltic action, there are scenarios—such as a full stomach, intestinal reverse peristalsis, or posture changes—that can result in reflux from the intestine to the biliary system. This can consequently lead to infections and form a "blind bag" or "dump pool" in the residual bile ducts, causing symptoms and pathological changes of cholangitis.
Madden's Animal Experiment
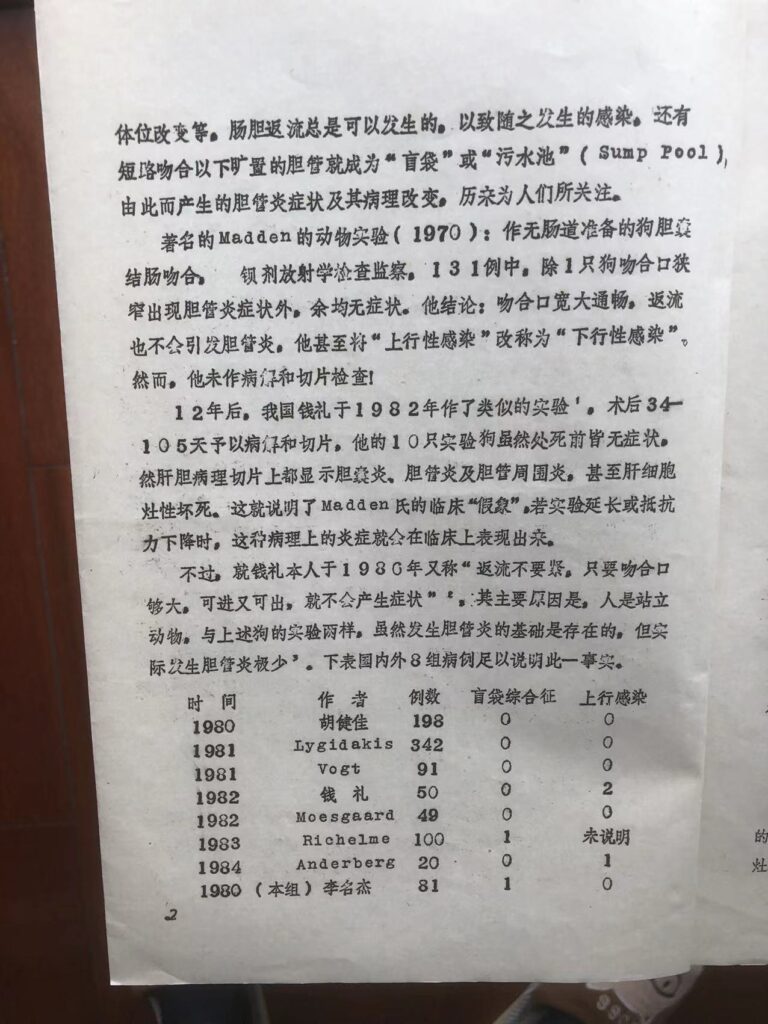
In a well-known animal study by Madden in 1970, gallbladder-colon anastomosis was performed on dogs without intestinal preparation. Of 131 cases monitored with barium radiography, only one dog showed symptoms of cholangitis due to anastomotic stenosis; the rest were asymptomatic. Madden concluded that a wide and open anastomosis would not result in cholangitis. He even shifted the terminology from "ascending infection" to "descending infection," although he did not perform pathological examinations.
Follow-Up Studies
Twelve years later, a similar experiment was conducted in China by Qian Li in 1982 [1]. Pathological examinations were conducted 34-105 days post-surgery. Though all 10 dogs were asymptomatic before being sacrificed, histological studies revealed cholecystitis, cholangitis, pericholangitis, and even focal hepatocyte necrosis. This unveiled the clinical "illusion" in Madden's study, suggesting that such pathological inflammation could become clinically significant if the experiment were prolonged or if immune resistance were lowered.
However, Qian Li himself later stated in 1980 that "reflux is not a concern as long as the anastomotic opening is large enough to allow bidirectional flow; symptoms will not occur" [2]. He attributed this mainly to the bipedal nature of humans, contrasting them with the quadrupedal dogs used in the experiments. Although the potential for cholangitis exists, actual occurrences are minimal [3]. This is supported by data from eight different case groups, both within China and internationally.
|
Year
|
Operator
|
cases
|
Blind Bag Syndrome
|
ascending infection
|
|
1980
|
Hu Jianjia
|
198
|
0
|
0
|
|
1981
|
Lygidakis
|
342
|
0
|
0
|
|
1981
|
Vogt
|
91
|
0
|
0
|
|
1982
|
Qian Li
|
50
|
0
|
2
|
|
1982
|
Moesgaard
|
49
|
0
|
0
|
|
1983
|
Richelme
|
100
|
1
|
(no info)
|
|
1984
|
Anderberg
|
20
|
0
|
1
|
|
1980
|
(this group)
Li Mingjie
|
81
|
1
|
0
|
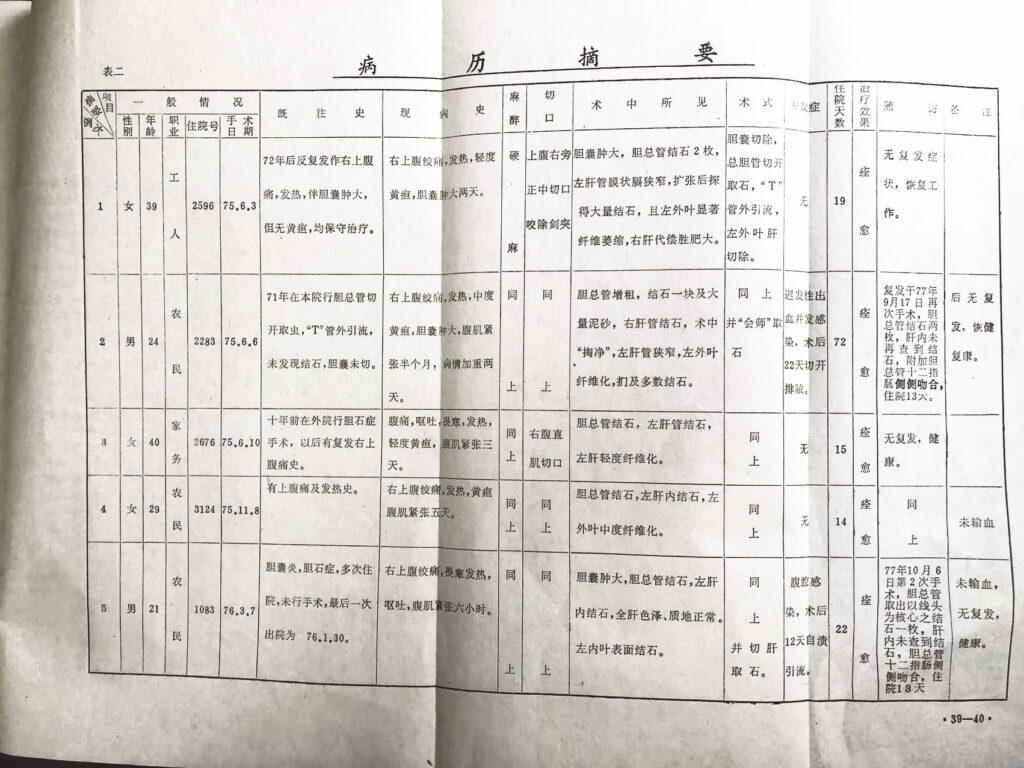
In this cohort of 441 secondary biliary surgeries, 81 cases involved Biliary-Intestinal Drainage (Bid), making up 18% of the cases [4]. The procedures included:
- 56 choledochoduodenal side-to-side anastomoses, of which 21 were secondary surgeries, one was a tertiary surgery, and 5 were end-to-side anastomoses.
- 2 Roux-Y hepaticojejunostomies
- 15 sphincterotomies of the Oddi sphincter, with six of these being secondary surgeries and one being a tertiary surgery.
- 2 Brown's cholangiojejunostomies
- 1 U-tube choledocho-intestinal bridging surgery
In this group, there were no instances of severe ascending infections post-Bid. However, one case of choledochoduodenal side-to-side anastomosis required a subsequent surgery due to a "test tube phenomenon," which was confirmed to be due to intrahepatic calculi falling two years post-operation [4].
Extensive practice has shown that as long as the Bid (Biliary-Intestinal Drainage) anastomotic site is wide, concerns about reflux are generally not a deterrent for surgeons. However, unfortunate cases do arise where, 2-3 years post-surgery, symptoms develop due to anastomotic narrowing caused by inflammatory proliferation. This has led to a variety of surgical innovations aimed at preventing anastomotic constriction and eradicating reflux. These innovations include the elongation of drainage intestinal tubes—sometimes up to 60 cm [5]. For targeted drainage, two parallel artificial intussusceptions are created on an open intestinal loop. These intussusceptions, along with parallel segments of bile and intestinal input loops, are then sealed to form a true Y-shaped, rather than T-shaped, anastomosis [6-10].
In light of the specific pathology of hepatolithiasis, it's recommended to perform a significant dissection of the extrahepatic bile duct and potentially extend it to the left and right hepatic ducts. This facilitates stone removal and stenosis alleviation, followed by a large-caliber side-to-side gallbladder-intestinal anastomosis, known as the Longmire-type operation, effectively preventing long-term postoperative stenosis. To eliminate the "blind pouch," a posterior duodenal foramen low choledochoduodenostomy is performed [2]. For physiological conformity and to reduce the incidence of gastrointestinal ulcers, a jejunal interposition is done to restore natural bile flow. To further facilitate future stone removal and biliary tract clearance, a subcutaneous blind loop (SB-jicd) is added [9].
Factors Related to the Efficacy of Bid (Biliary-Intestinal Drainage)
1. Incomplete Cure of Primary Disease
Bid serves the purpose of clearing bile flow but does not act as a substitute for treating the underlying primary disease. The surgery aims to completely remove gallstones, Ascaris lumbricoides, and manage primary lesions or complications in the liver, gallbladder, and pancreas. Despite initial optimism that intrahepatic stones would naturally pass through internal drainage, clinical evidence proves otherwise. In instances where intrahepatic calculi "collapse," they may obstruct the anastomotic site, causing symptoms. When biliary constriction above the anastomotic site is not corrected or eliminated, bile-intestinal reflux becomes difficult to manage, leading to challenging infections. In cases of malignancy, the focus is either on curative or palliative surgical approaches. For congenital choledochal cysts, removal of the cyst followed by Bid is advisable to prevent the cyst wall from becoming inflamed or malignantly transformed.
In the early stages, due to the Finster procedure's ease of operation and good short-term outcomes, there was a tendency to overuse it, accounting for 70% of Bid cases in this study group. Diagnostic capabilities at the time, such as imaging and direct cholangiography, were not as advanced, leading to an incomplete understanding of the pathology. This often resulted in neglecting the treatment of intrahepatic lesions and bile duct stenosis, subsequently causing a high reoperation rate of 13.2%, and in some cases, three or four subsequent surgeries. However, with the advent of Percutaneous Transhepatic Cholangiography (PTC), the use of Bus Ultrasound (BUS), and an improved understanding of the disease, surgical techniques advanced, leading to better outcomes.
2. Choice of Timing for Surgery
It is generally advised against performing emergency primary drainage (Bid). This recommendation is based on multiple factors. First, emergency surgeries for acute or severe conditions should not be complicated due to the immediate need for treatment. Second, the short time frame makes it challenging to gain a comprehensive understanding of the condition, thus complicating the decision for the optimal surgical approach. Lastly, performing Bid during the stage of inflammatory edema could reduce its safety and increase the likelihood of long-term restenosis.
However, there's a school of thought advocating for completing Bid in a single stage, thanks to advancements in diagnostic technologies. With the use of Bus, PTC, ERCP, CT, and choledochoscopy, a more accurate understanding of the condition is possible, allowing for more informed surgical choices. This avoids complications related to anatomical disarray, adhesions, and accessory injuries in case of a second surgery, thus minimizing the patient's physical and financial burdens.
In summary, the choice of surgical approach should be made after comprehensive consideration of several factors: the local anatomical conditions, the patient's overall ability to endure surgery, and both the short-term and long-term needs dictated by the disease condition.
3. Issues with Technology Implementation
The approach to biliary-enteric anastomosis has evolved significantly. Initially, the focus was solely on ensuring free bile flow. However, with time and lessons learned from clinical experience—sometimes at a cost—there's now a shift towards understanding the postoperative physiological and pathological changes in the body. This is considered a valuable progress in the field.
Technical Precautions and Best Practices
-
Preventing Anastomotic Stenosis: It's crucial to create a spacious channel for bile flow and to avoid performing this surgery during periods of inflammation.
-
Understanding Blood Supply: Given that the blood supply to the extrahepatic bile ducts is axially distributed, excessive separation of the bile ducts should be avoided to prevent ischemic stenosis caused by surgical trauma.
-
Suture Techniques: Leakage of bile between different layers of bile duct tissues can hinder tissue healing. Therefore, suturing should be done in a tension-free manner to prevent this.
-
Optimizing Duct Length: The non-functioning segment of the bile duct should be kept as short as possible to minimize the formation of blind pouches.
-
After Bid: Post-Bid, the regulatory function of the sphincter of Oddi is lost, leading to decreased pressure in the bile ducts. In this condition, the gallbladder merely serves as a diverticulum. Given that the cystic duct is small and convoluted, ongoing gallbladder inflammation and stone formation are almost inevitable. Therefore, it's recommended to remove the gallbladder when performing Bid.
4. Selection of Surgical Procedures and Principles of Joint Observation
With the abundance of Bid surgical procedures, how do we choose among them? In addition to considering patient conditions, pathology, available equipment, technical conditions, and the physician's personal experience, several principles and requirements are emphasized:
- Biliary flow should be physiological: The surgery should aim to avoid disrupting the natural physiology and pH of the digestive system to minimize the risk of gastrointestinal ulcers.
- Shorten the non-functioning bile duct segment: The non-functioning parts of the bile duct should be minimized to avoid complications.
- Fewer short-term symptoms: The surgical method should have fewer immediate complications.
- Low risk of restenosis: The surgery should minimize the risk of the internal drainage becoming narrow again.
- Minimal "ascending infection": The chosen method should minimize the risk of infection moving upward in the system.
- Complexity and safety of the operation: The surgical method should balance complexity against safety.
- Favorable for monitoring and re-examination: Post-operative follow-up should be facilitated by the surgical method chosen.
Based on the aforementioned principles, the best surgical approach is chosen depending on the patient's condition.
- SB-jicd: This method is generally the first choice for cases with multiple intrahepatic and extrahepatic stones to avoid the need for multiple surgeries.
- Jied: For non-stone-related benign obstructions in the biliary tract, the Jied procedure is advisable to restore physiological conditions.
- Finster Surgery: For older patients with severe diseases, the Finster operation may be suitable. If conditions allow, this can be an alternative approach.
- Oddi Sphincterotomy or Plasty: For obstructions in the far end of the common bile duct or stenosis at the outlet, these procedures may be performed.
- Roux-en-Y Biliary Bypass: This method reduces the neutralizing effect of bile on gastric acid within the duodenum. There are claims that this could lead to an ulcer rate as high as 52%, although clinical observations put it at around 10%. Pappa-Lardo recommends an additional procedure (possibly a specific type of cut or incision, as the term "迷切" is not entirely clear, 建议此术附加迷切) to be included in the surgery. This suggestion, however, hasn't garnered much attention in China, where the surgical method in question is still widely used. One speculation for this could be that gastric acid levels are generally lower in the Chinese population compared to Western countries.
-
Endoscopic Sphincterotomy (ES): This surgical technique avoids the need for open abdominal surgery and represents a recent advancement in foreign countries. However, it hasn't gained widespread adoption in China yet, possibly due to limited experience with the procedure.
Comments on Several Commonly Used Surgical Procedures
I. Sphincterotomy and plasty of Oddi
In the case of Oddi sphincterotomy and plasty, the surgical procedure theoretically aligns with the natural flow of bile and eliminates the presence of a 'blind bag,' making natural stone expulsion possible. In this particular study, 15 cases were performed, accounting for 20% of all biliary-intestinal diversion (Bid) procedures. Post-operative ascending infections were observed in two cases, which were controlled using antibiotics.
Due to advancements in endoscopic technology, especially abroad, there's a shift towards duodenal endoscopic sphincterotomy (ES). This method avoids the need for a laparotomy and has a high stone-removal rate of 85-90%. However, the complication rate is also noted to be 28%.
When an incision of 10mm is made in the Oddi sphincter, it relieves muscle spasms but doesn't entirely remove the functionality of the distal bile duct sphincter. This makes it prone to restenosis, making it difficult to achieve the desired long-term outcome.
In terms of the distal sphincter, a more extended cut could result in complete severing of the ampullary and most of the common bile duct sphincter. The consequences of such cuts need to be weighed carefully, particularly in terms of potential for bile reflux and ascending infections.
Considering that the function of the distal sphincter of the bile duct comprises three components—the Oddi muscle, the inner wall sphincter of the bile duct, and the partial function of the circular muscle in the duodenum—if an incision of 1.5 cm is made, it would sever the entire ampulla and a large portion of the common bile duct sphincter. If the incision extends to 2.5-3 cm, all three components would be severed, essentially resulting in a low-position choledochoduodenostomy. Any incision of these various lengths must be done cautiously to prevent damage to the pancreatic duct. Moreover, due to the pressure equilibrium between the bile and intestinal tracts, reflux from the intestine to the bile duct is almost inevitable. This could easily lead to ascending infections. Additionally, there's the issue that a dilated common bile duct greater than 20 cm can still form a funnel-shaped narrow segment post-surgery.
Choi, in 1982, proposed a re-operative extraperitoneal approach to avoid the difficulties of adhesions and collateral damage encountered when dissecting the original surgical area.
Plasty involves the removal of a wedge-shaped portion of the anterior lateral wall of the common bile duct outlet, followed by suturing. To prevent reflux, a valve was designed.
This operation, when used as an adjunct to other internal drainage procedures, has considerable value in eliminating the 'blind bag.' Four such cases were noted in this study, and in one case, liver stones were no longer present two years post-operation, possibly a supporting case for the long-term efficacy of the procedure.
II. Choledochoduodenostomy
This procedure involves two types of anastomosis: lateral-lateral and terminal-lateral. The operation is simple, straightforward, and safe, with good short-term recovery. Influenced by the "illusion" created by Madden's experiments, this procedure was widely performed in earlier years. Among our group of 81 cases, this technique was applied in 61 cases, making up 75%. However, recent consensus—built upon observations from reoperations, insights from animal experiments, and a deeper understanding of the pathophysiology of the biliary tract—indicates that the appropriateness of this surgery has significantly decreased.
Particularly problematic is the classic Finster's fissure technique, which has several downsides: the anastomosis is narrow, there's a latent risk of retrograde infection and blind-end syndrome, and prolonged exposure to digestive juices can induce chemical cholangitis that leads to mucosal atrophy. This results in goblet cell and fibrous tissue proliferation, making the duct wall thick and hard. Post-anastomotic biliary infections often involve a complex mix of aerobic and anaerobic bacteria, complicating treatment. Sometimes, extreme measures like a B-II partial gastrectomy are required to divert food, or the posterior wall of the blind end needs to be cut open, or a new biliary-intestinal anastomosis has to be constructed.
The procedure is generally not recommended for those with hepatogenic stones that haven't been completely removed or if there's uncorrected bile duct stenosis above the anastomotic site. For gallstones combined with lower common bile duct narrowing, often termed "Western-style gallstones," this procedure can be the best option. It's also a viable choice for elderly or frail patients who can't endure complex surgeries.
To overcome the limitations of this technique, various improved methods have been introduced recently, including post-duodenal choledochoduodenostomy and hollow-end biliary anastomosis. These improvements are theoretically more sound and have shown good results in practice.
III. Biliary-Jejunal Roux-en-y Anastomosis
One issue with this technique is that extending the jejunal loop used for bile drainage to even 60 cm doesn't necessarily eliminate the risk of reflux infection. Directly routing bile into the jejunum disrupts physiological norms. This not only hampers the digestion and absorption of fats but also reduces the suppression of gastric juice secretion in the upper jejunum. For those with high gastric acid levels, the absence of bile to neutralize stomach acid in the duodenum can increase the incidence of ulcer disease. Additionally, an overly long jejunal loop can twist and adhere, causing potential obstructions. Changes in the functionality of this intestinal segment make it difficult to maintain a normal microbiota, giving rise to a condition known as "jejunal blind loop syndrome."
Despite these challenges, this remains one of the most frequently used surgical methods. It allows for tension-free anastomosis with bile ducts at all levels, including the Longmire procedure. This versatility addresses issues like intrahepatic bile duct stenosis and enables the reconstruction or palliative bypass of the biliary-intestinal pathway following substantial resection of malignant liver tumors. Ongoing technical improvements aim to minimize the risk of reflux infection as much as possible.
IV. Intermittent Jejuno-Biliary-Duodenal Anastomosis (Jicd)
This surgical technique evolved from the Roux-en-y procedure. It was first reported by Grassi in 1969 and subsequently introduced in China by Shiweijin in 1982. The method involves interposing a segment of the jejunum between the bile duct and the duodenum, aiming to restore the physiological state of bile flow. This addresses some of the limitations associated with the Roux-Y method. Regarding the length of the interposed segment, Grassi recommended 20 cm, while Huang Zhiqiang advised against excessive length. An artificial nipple is designed at the distal end of the interposed jejunum and is inserted into the wall of the duodenum during anastomosis.[9] Shi Weijin suggests that a 60 cm length could essentially prevent reflux. Technically, attention must be paid to the "peristaltic direction" when placing the interposed intestinal segment. End-to-side anastomosis between the bile duct and jejunum is preferable as it allows for more flexible design of the anastomotic site.
However, the procedure comes with three anastomotic connections, making it more invasive and complex compared to the Roux-Y method, which involves two anastomotic sites, and choledochoduodenostomy, which has just one. This complexity has hindered its widespread adoption. Despite these challenges, the technique is currently being promoted in China due to its advantages. As it has not been in use for a long period, its long-term efficacy and ultimate evaluation still require further clinical validation.
V. Subcutaneous Blind Loop Interposition of Jejuno-Choledochoduodenal Anastomosis (SB-JICD)
This technique evolved from the aforementioned JICD and is specifically designed for cases where multiple intrahepatic stones are difficult to remove completely or where hepatic stones are expected to regenerate. The subcutaneous blind loop is reserved for direct access when needed to remove stones, worms, or facilitate bile drainage. It can also serve as a route for medication administration and postoperative monitoring.
Built upon the foundation of Roux-Y and JICD procedures, this technique involves interposing a segment of jejunum, which is then subcutaneously buried and marked with a silver clip. Corresponding skin surface markings can also be made for easier monitoring and treatment access. A blind loop length of around 10 cm is recommended to minimize the risks associated with "blind loop syndrome."
However, this procedure has not yet gained widespread acceptance. It leaves another option for suitable candidates, but it comes with its own set of challenges. Not only is the surgery complex, but the risk of infection in the blind loop also exists. Furthermore, the procedure may not be as effective in practice as it is in theory, especially for deeper hepatic lesions. Even if a cholangioscope is inserted through this route, it may not necessarily solve the problem.
VI. Others
Other techniques like gallbladder-gastrointestinal anastomosis are generally discarded due to the circuitous and narrow nature of the gallbladder duct, which cannot ensure reliable drainage. These methods are no longer considered viable options, especially in the case of late-stage malignant tumors or critically ill elderly patients. In our early practice, we performed a few gallbladder-stomach and gallbladder-jejunum anastomoses. These techniques played an active role in alleviating symptoms for patients with distal biliary obstruction-induced jaundice, such as those with late-stage pancreatic head cancer.
References:
-
Qian Li: Analysis of the pathogenesis of secondary cholangitis after biliary-intestinal anastomosis and the efficacy of various biliary-intestinal internal drainage procedures. Anthology of Papers on Cholelithiasis, Wenzhou Medical College, 1982.
-
Qian Li: Treatment of Primary Pigment Stones in the Common Bile Duct. Journal of Practical Surgery, 1986; 1:19.
-
Zhang Shengdao: Evaluation of choledochoduodenostomy in the treatment of severe acute cholangitis. Journal of Practical Surgery, 1986; 6(1): 42.
-
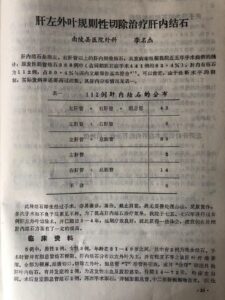
Li Mingjie: Hepatectomy for treating intrahepatic gallstones. Domestic Medicine, 1980 #161; Wannan Medical Journal, 1980, 13:51-55.
-
Shi Weijin: Indications and evaluations of JICD and SB-JICD. Journal of Practical Surgery, 1986; 6(1): 44.
-
Tan Yuqian: Evaluation of Roux-Y type cholangiojejunostomy. Journal of Practical Surgery, 1986; 6(1): 44.
-
Zhang HD: An Exploration on the prevention of Reflux in "Y" Type Choledochojejunostomy. Abd 'surg, 1985; 27:34.
-
Kassi M: Improved technique of end-to-side anastomosis of the intestine. SGO, 1974; 138:87.
-
Huang Zhiqiang, et al.: Artificial nipple-type intermittent jejuno-biliary-duodenal anastomosis. Journal of Practical Surgery, 1986; 6(1): 48.
10. Wang Xunying: Directional drainage surgery for the common bile duct and jejunum. Chinese Journal of Surgery, 1980; 18:320.
11. Choi TK Ann: Snrg, 1982; 196: 26.
This article was originally published in Proceedings of the Second Annual Surgical Conference of the Third Session in Anhui Province,Sept. 1988;87
Changhang Hospital, Li Mingjie
【李名杰从医67年论文专辑】(电子版)
【李名杰从医67年论文专辑(英语电子版)】